[vc_row][vc_column][vc_simple_slider ids=”6868″][ultimate_spacer height=”30″][vc_column_text]
- Respect for human dignity and human rights is the ethical foundation of everything we do.[1]
- We are inspired by the opportunity to address unmet medical needs for patients living with life-threatening diseases around the world.[2]
- We aspire to improve the health and wellness of people worldwide and to expand access to our medicines and vaccines.[3]
- We are passionate about transforming patients’ lives. We commit ourselves to scientific rigor, unassailable ethics, and access to medical innovations.[4]
- We do more than treat diseases—we aim to make a remarkable impact on people’s lives.[5]
These are excerpts from the values of pharmaceutical companies that are global leaders in inventing and producing many essential medicines, including HIV / AIDS antiretroviral drugs.
With these values, the companies position and introduce themselves to the world.
They produce medicines that can save lives and at the same time artificially restrict access to these drugs for financially deprived people and for countries that fall outside their commercial interests.
“We did not develop this medicine for Indians.”
We developed it for Western patients who can afford it ‘
Marijn Dekkers – Bayer CEO in 2010 – 2016
Thanks to the decades-long existence of effective antiretroviral medicines, HIV/AIDS is no longer considered to be a fatal disease. A timely and regular administration of these drugs ensures that a human life is not endangered.
However, despite the inspiring values on websites, artificial barriers created by these pharmaceutical companies are one of the main reasons that millions of people die every year worldwide, because of HIV / AIDS only because they have no access to medications.
Why?
Because a human’s life costs less than a medicine which can save his or her life.
Pharmaceutical companies are artificially maintaining high prices for essential drugs. The barriers created by them are mainly related to the establishment of monopolies on the market and the restriction of production of generic medicines and their access to the market through protecting patent rights and extending them as much as possible.
What is happening in Georgia?
HIV / AIDS treatment in Georgia has been available since 2004 with the financial support of the Global Fund to Fight AIDS, Tuberculosis, and Malaria, whereby treatment is provided free of charge to all people who are diagnosed and registered in the national program.
The procurement of medications within the programs is carried out by the Global Fund’s Pooled Procurement Mechanism (PPM).
PPM is a strategy designed to create an economically favorable and efficient mechanism for procuring essential medicines.
Due to the volumes of procurements proceeded by the Global Fund, PPM creates opportunities for financial savings and a significant decrease of prices of medications.[6]
The key principle of this mechanism lies on ‘’Framework Agreements’’ with ARV manufacturing pharmaceutical companies that defines pre-negotiated favorable prices within procurement carried out by the Global Fund. While using this mechanism, a country can avoid the patent rights of pharmaceutical companies and the restrictions imposed by them.
However, due to the recent developments, Georgia faces significant challenges, which can cause significant barriers to the access of HIV treatment.
As a result of the renewal of the countries’ classification system according to their income level by the World Bank[7] in 2014; as well as the introduction of a new funding model (NFM) [8] by the Global Fund to Fight AIDS, Tuberculosis and Malaria, Georgia belongs to so-called transitioning countries in terms of funding[9]. This entails the gradual reduction in funding by the Global Fund and the need to increase state allocations, including for procurement of HIV / AIDS ARV medicines.
Under the framework of state funding, the issue related to procurement mechanisms of medications comes to the agenda. In particular, through which mechanism and, most importantly, at what price the medications will be procured.
Georgian legislation in the field of state procurement, regulation of intellectual property rights and patent rights is not sufficiently flexible to ensure the procurement of quality drugs at favorable prices, to promote market competition and to open access to generic medications as well as to create opportunities for using international mechanisms for reducing drug prices.
This challenge is accompanied by the commitments under the Association Agreement (AA)[10] signed between Georgia and the European Union in 2014, which obliges the country to carry out the relevant legislative amendments directly aimed at creating favorable conditions for the brand pharmaceutical industry.
These legislative amendments include additional measures to protect patent rights on pharmaceutical products, in particular, to extend patent terms and to ensure so-called data exclusivity to guarantee the confidentiality of information and to prevent its usage by third parties thus directly limiting access to the local market for the generic manufacturers.
Most of the legislative amendments relating to the commitments undertaken within the AA were implemented in 2017[11]. These amendments pose a significant threat to the availability of drugs, including HIV antiretroviral medications, especially under state procurements.
What reality may we face?
HIV antiretroviral medications have been procured by allocations from the state budget since 2016.
The procurement of drugs with state budgetary sources is also carried out by using the Global Fund’s mechanism which, temporarily allows a country to avoid potential challenges. However, the main remaining questions are:
- whether this mechanism will remain available for the use after the country’s transition from the Global Fund
- and whether the country will be able to use the same benefits, including, to evade patent rights
Georgia, as a country with a low disease burden of HIV infection and, accordingly, with a low purchase power is not commercially interesting for pharmaceutical companies. Therefore, they will try to set the highest possible prices for medications to maximize their profits.
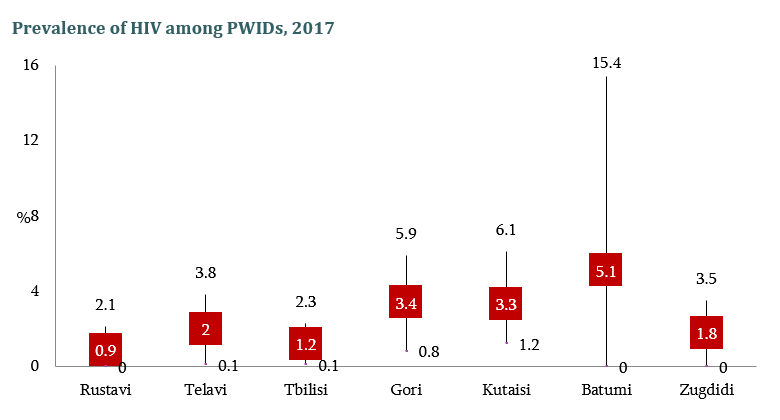
Taking into consideration that the incidence of HIV infection in the country is rising over years, this can become a quite heavy burden for the state budget.
To illustrate, we can compare prices of drugs procured by the Global Fund mechanism in Georgia with prices of the same drugs in other countries purchased under state procurement:
|
Georgia (Global Fund Mechanism) |
Poland
(State Procurement) |
Latvia
(State Procurement) |
|
Unit Cost
$ |
Package Cost
$ |
Unit Cost
$ |
Package Cost
$ |
Unit Cost
$ |
Package Cost
$ |
| Abacavir 300mg tablet |
0.1832 |
10.99 |
3.8125 |
228.75 |
3.4702 |
208.21 |
| Abacavir + Lamivudine (combined drug) 600/300mg tablet |
0.4163 |
12.49 |
14.1667 |
425 |
11.619 |
348.57 |
| Atazanavir 300mg capsule |
0.6 |
18 |
15.4167 |
462.5 |
14.8337 |
445.01 |
| Darunavir 600mg tablet |
1.667 |
70 |
11.025 |
661.5 |
11.6655 |
699.93[12] |
This data is a clear illustration of what realities we may face and how big the rise in the level of expenditures we will have to deal with.
In countries indicated in the table as examples (Poland, Latvia) high prices on medications are exactly due to monopolies of pharmaceutical companies and patent restrictions which limit the availability of generic medicines on the market, restrict competition and decrease in prices of drugs.
To avoid similar developments in the country, it is important to immediately start working on changes in local legislation to create a favorable environment in terms of the availability of drugs and to establish a legal framework which will allow for making use of internationally recognized mechanisms for reducing prices of medications.
Health is a fundamental human right, that also covers access to essential lifesaving medicines. The invention of the medication and its physical existence does not mean access to it. We live in an environment where human life is in danger due to the greed of the pharmaceutical industry, where a human life depends on how much money an individual has. The state is obliged to provide a person with the right to health!
[1] https://www.bayer.com/en/our-values.aspx
[2] http://www.gilead.com/about/ethics
[3] http://www.merck.com/about/home.html
[4] https://www.roche.com/about/our_purpose.htm
[5] https://www.abbvie.com/our-company/about-abbvie.html
[6] https://www.theglobalfund.org/en/sourcing-management/health-products/
[7] https://datahelpdesk.worldbank.org/knowledgebase/articles/378834-how-does-the-world-bank-classify-countries
[8] https://www.theglobalfund.org/en/funding-model/
[9]https://www.theglobalfund.org/media/5641/core_projectedtransitionsby2025_list_en.pdf?u=636649300140000000
[10] http://www.parliament.ge/uploads/other/34/34754.pdf
[11] http://www.sakpatenti.gov.ge/media/page_files/patent_law_2017_Iy62qmS.pdf
[12] http://arv.ecuo.org/[/vc_column_text][/vc_column][/vc_row][vc_row][vc_column width=”1/1″][ultimate_spacer height=”30″][/vc_column][/vc_row]
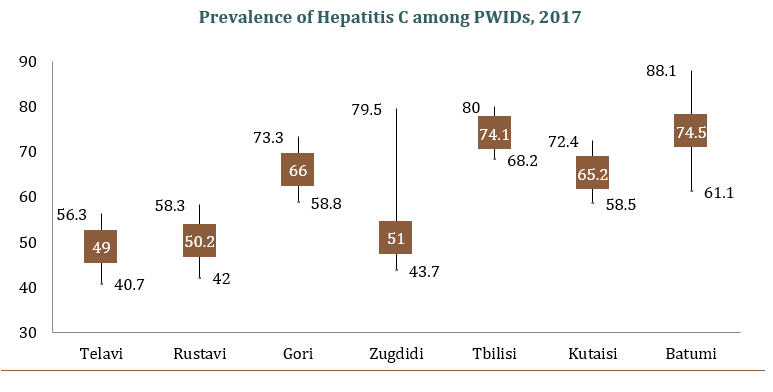 D is much higher compared to HIV.
D is much higher compared to HIV.